


Review
History
• Medication: Clopidogrel, Atorvastatin, Valsartan and hydrochlorothiazide.
• 药物:氯吡格雷,阿托伐他汀,缬沙坦氯吡格雷。
• 神经查体:(-)
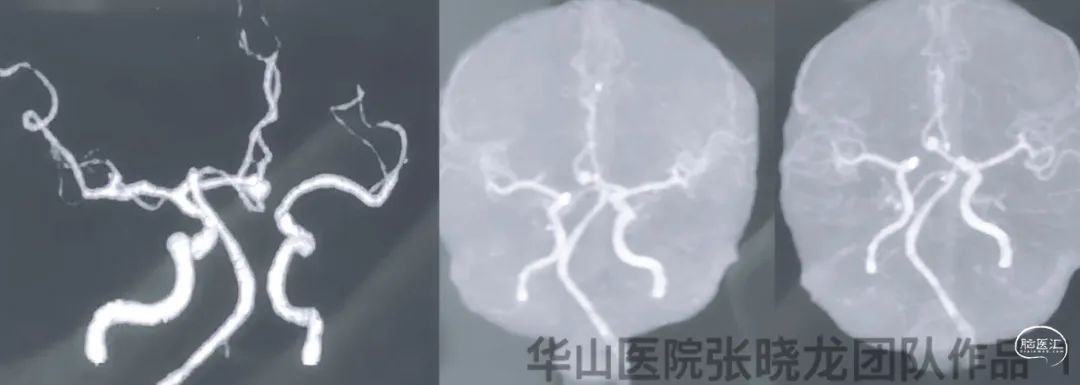

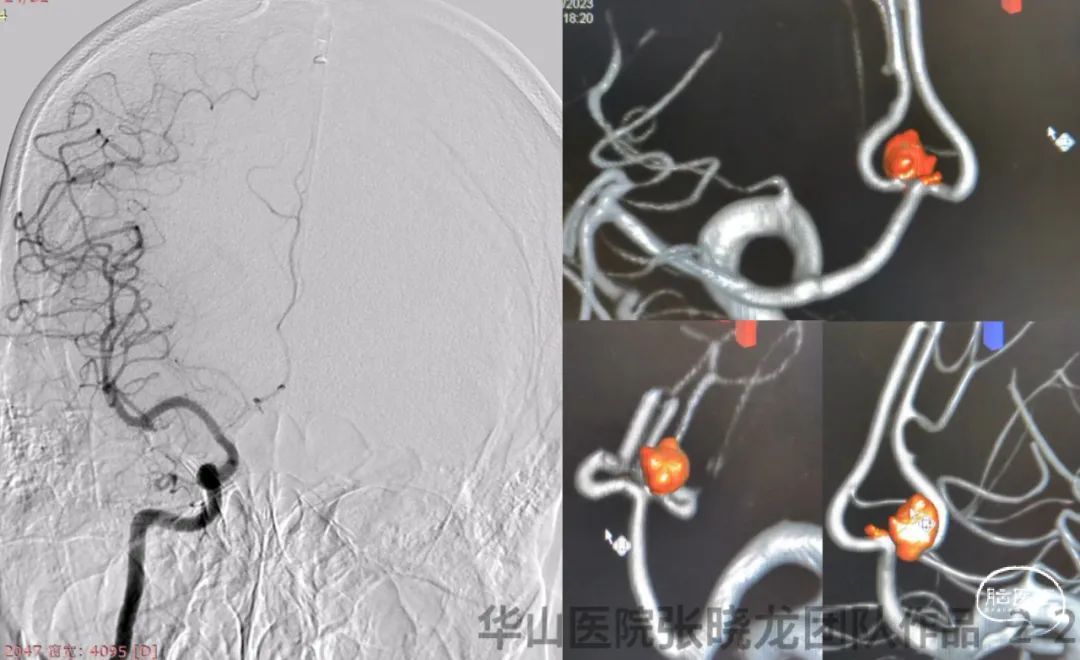
图 2 GIF. DSA和3D重建示左侧A2段不规则动脉瘤,旁边有一枚微小前交通动脉瘤。左侧颈内动脉颈段夹层,右侧A1段发育不佳。
1
Strategy
• A tiny irregular anterior communicating aneurysm was treated by stent remolding technique because coils may be difficult to insert into. A Solitaire stent will be selected.
• Due to right A1 underdeveloped, the anterior communicating artery must be preserved.
• Left ICA cervical segment dissection can be treatment by a carotid stent.
• 前交通动脉微小不规则动脉瘤,弹簧圈填塞困难,计划采用Solitaire支架重塑作用治疗。
• 由于右侧A1发育不佳,前交通动脉必须保留。
• 左侧颈内动脉颈段夹层可采用颈动脉支架治疗。
2
Operation
Figure 3 GIF. General heparinization was performed. An size 4.5*4.3mm, neck 2.9mm, proximal parent artery 2.9mm, distal parent artery 2.0mm. 6F Envoy DA was placed into left ICA cavernous segment. Nimodipine 1ml was administered. First advanced a C-tipped Freepass-21 into left A2, then SL-10 into right A2. Tried to exchanged SL-10 to another Freepass-21, Rebar-18 and Prowler plus, all failed. Withdrew the Freepass-21 of left A2 segment. A Frepass-21 was place at the right A2 segment, then navigated a SL-10 into the left A2 via a V-18 for support. A Solitaire 4*20mm was deployed from right A2 to left A1.
图 3 GIF. 行全身肝素化。测量动脉瘤大小4.5*4.3m,瘤颈2.9mm,近端载瘤动脉直径2.9mm,远端载瘤动脉直径2.0mm。将6F Envoy DA导引导管置于左侧颈内动脉海绵窦段,经导引导管给予尼莫地平1ml。将Freepass-21微导管(头端塑C弯)后超选至左侧大脑前动脉A2段,SL-10微导管超选至右侧A2。选用另一枚Freepass-21微导管交换SL-10微导管,导引导管不能兼容。更换Rebar-18和Prowler plus微导管均不能兼容。遂撤回左侧大脑前动脉Freepass-21。将Freepass-21微导管置于右侧A2,在V-18支撑下将SL-10置于左侧a2。选用Solitaire 4*20mm于右侧A2至左侧A1释放。

图 4 GIF. SL-10微导管头段塑C弯后置于动脉瘤腔内。经微导管填入Target 3D 5mm*15cm弹簧圈,Atlas 3*21mm支架从左侧A2向A1释放,随后继续填入3枚弹簧圈(target 3D 4mm*15cm, 4mm*10cm, 4mm*8cm)。复查造影动脉瘤栓塞满意,前交通动脉通畅。经导引导管内静注替罗非班10ml和尼莫地平1ml。
图 5 GIF. Precise 6*40mm支架覆盖颈段夹层。


图 6 GIF. 复查造影A2段动脉瘤不显影,颅内血管通畅。
图 7 GIF. 术后复查Dyna-CT未见出血。
3
Post-Operation
• Medication:
1. Tirofiban 7ml/h and 4ml/h maintained for 24h respectively.
2. Aspirin and Clopidogrel were prescribed.
3. 阿司匹林抑制率92.1%,氯吡格雷抑制率96.8%,氯吡格雷基因代谢中等代谢,酶活性偏低。
Video 1. The aneurysms were not relapsed and parent artery was patent by 9 month follow up.
视频 1. 9个月随访动脉瘤无残余及复发,载瘤动脉通畅。
视频 2. 9个月随访前交通微小动脉瘤未见显影。

图 8. 载瘤动脉被Solitaire支架拉直明显。
视频 3. 9个月随访颈段夹层完全修复。
4
Summary
• A relative large irregular dissecting aneurysm located at the left A2segment harbored a high rupture risk, which was suggested treatment. Due to wide neck, stent assisted coiling technique was adopted.
• A tiny irregular anterior communicating aneurysm was treated by stent remolding technique because coils may be difficult to insert into. A Solitaire stent was selected. The small aneurysm was invisible because the parent artery was straightened by a Solitaire stent.
• Envoy DA can not compatible with a Frepass-21, a Rebar-18 and a Prowler Plus. Therefore SL-10 was selected, and Atlas stent assisted large coiling was adopted.
• Due to right A1 underdeveloped, the anterior communicating artery must be preserved.
Dangerous points:
• The tiny aneurysm ruptured during right A2 segment super-selection.
• 左侧A2段相对较大的不规则夹层动脉瘤有破裂风险,建议治疗。动脉瘤瘤颈较宽,采用支架辅助栓塞。
• 前交通动脉微小不规则动脉瘤,弹簧圈填塞困难,采用了Solitaire支架,通过支架重塑作用治疗。小的动脉瘤随访消失是由于Solitaire支架的拉直效应。
• Frepass-21, Rebar-18和Prowler Plus微导管均与Envoy DA不能兼容,所以选择SL-10微导管,左侧A2动脉瘤采用Atlas辅助大圈技术栓塞。
• 由于右侧A1发育不佳,前交通动脉必须保留。
该病例治疗危险点:
• 右侧A2超选时微小动脉瘤有破裂风险。
• 左侧A2动脉瘤栓塞时载瘤动脉有闭塞风险。
声明:脑医汇旗下神外资讯、神介资讯、脑医咨询、Ai Brain 所发表内容之知识产权为脑医汇及主办方、原作者等相关权利人所有。
投稿邮箱:NAOYIHUI@163.com
未经许可,禁止进行转载、摘编、复制、裁切、录制等。经许可授权使用,亦须注明来源。欢迎转发、分享。
投稿/会议发布,请联系400-888-2526转3。

