


原作出处:Dahl RH, Eskesen V, Poulsgaard L, Krogager ME, Benndorf G. Transfistulous coil occlusion of high-grade tentorial dural arteriovenous fistulas: An effective alternative to liquid embolic agents. J Neuroradiol. 2026 Mar;53(2):101528. doi: 10.1016/j.neurad.2026.101528. Epub 2026 Feb 1. PMID: 41633475.
以下为AI解读,仅供参考。
硬脑膜动静脉瘘(DAVF)是常见颅内血管畸形,高级别小脑幕DAVF(Borden Ⅲ型、Cognard Ⅳ型)出血风险高,可致脑出血、静脉梗死、痴呆等严重并发症。目前主流治疗为经动脉液体栓塞剂(LEA)栓塞,但存在靶外栓塞、微导管嵌顿、瘘口闭塞不全等风险;传统经静脉逆行入路亦常受解剖限制。
经瘘口弹簧圈栓塞术(Transfistulous Approach,TFA)是一种经动脉途径超选穿过动静脉瘘口、直接抵达DAVF近端初级引流静脉起始部(即“瘘脚”),以弹簧圈致密填塞实现瘘口精准、可控闭塞的神经介入技术。本世纪初,Fukai、Tokunaga、Layton等即已相继证实经动脉超选静脉腔的可行性,但早期微导管难以通过高级别DAVF的迂曲瘘口路径,使这一精准策略沉寂多年。但是依托新一代1.3F低剖面微导管与三轴系统的结合,TFA得以焕发新生。通过精准锁定DAVF根治核心靶点,规避前述短板,TFA不仅有望成为高级别小脑幕DAVF安全高效的优选方案,并且在解剖条件适配时应考虑作为首选术式。
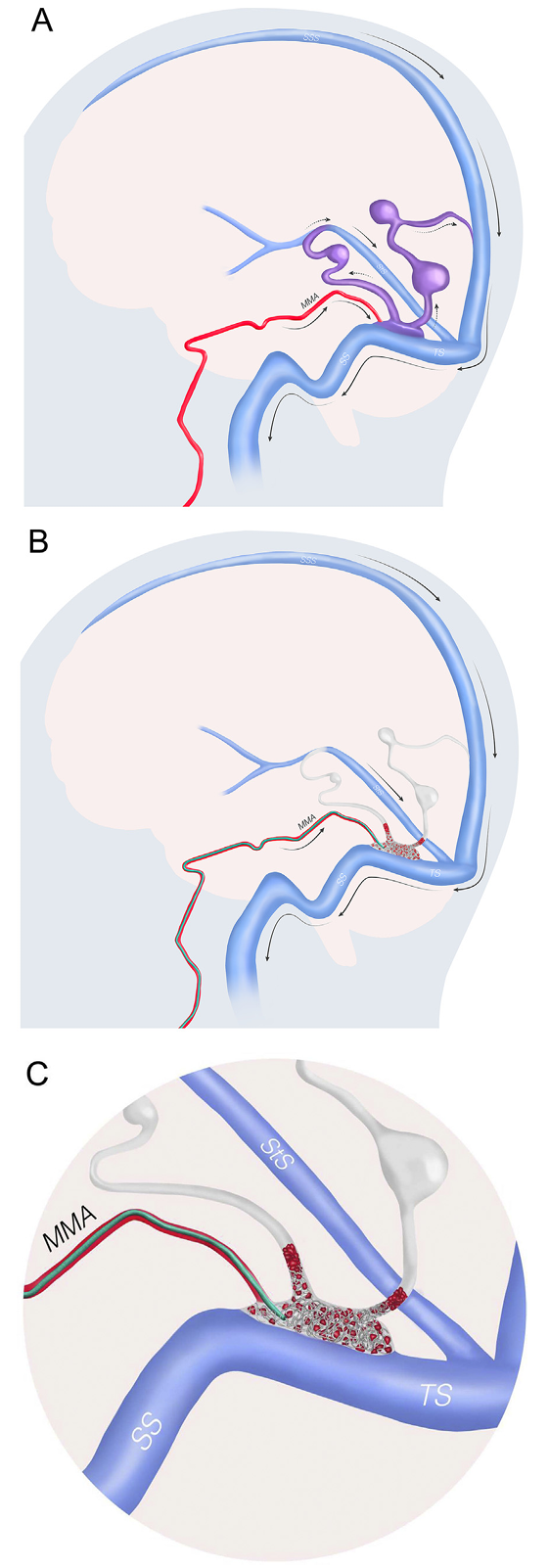
Fig. 3. Illustration demonstrating the transfistulous approach (TFA). A. Lateral view of a dural arteriovenous fistula supplied by the middle meningeal artery draining into both dilated cortical and deep veins with focal ectasias. The middle meningeal artery feeder connects to the so-called foot of the vein, consisting of the primary proximal venous drainage located in the tentorium near the transverse sinus. The direction of blood flow is shown by arrows. B. The TFA is performed by transarterial catheterization of the middle meningeal artery, navigating a low-profile microcatheter through the fistulous point into the proximal venous outlet, followed by deployment of coils. C. Enlarged view showing positioning of the microcatheter and coil deployment in the proximal venous outlet, causing thrombosis and occlusion of the fistula. When a two-directional proximal venous drainage is present, as shown here, both venous exits should preferentially be packed with coils. In patients with suitable anatomy, this approach may allow for complete fistula occlusion in a single session. The technique is particularly useful when enlarged arterial feeders are present, such as in patients with longstanding high-grade dural arteriovenous fistulas. MMA: Middle meningeal artery; SS: Sigmoid sinus; SSS: Superior sagittal sinus; StS: Straight sinus; TS: Transverse sinus.
1. 病变分型:Borden Ⅲ型、Cognard Ⅳ型高级别小脑幕DAVF
2. 关键解剖条件:
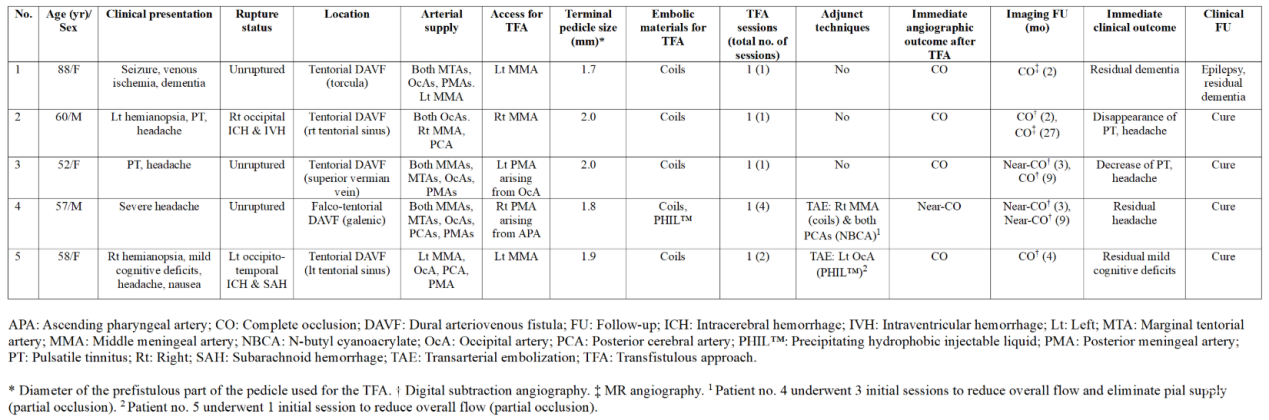
✔ 供血动脉主干增粗(平均直径1.9mm)
✔ 瘘口静脉腔适合弹簧圈填塞
✔ 直接向大脑/小脑静脉引流
3. 优选场景:逆行静脉入路困难/风险高;小脑幕窦、横窦、上矢状窦区DAVF
1. 通路与器械
✔ 入路:经股动脉三轴系统(8F Neuron MAX + 5F Sofia远端导管 + 1.3F Headway Duo微导管)
✔ 供血动脉入路:脑膜中动脉(3例)、脑膜后动脉(2例)
✔ 弹簧圈规格:Target XL(Stryker)、HydroCoil 18(10mm×31cm,Terumo)
2. 麻醉与影像
✔ 全麻、ACT>250秒肝素化
✔ 3D-DSA精准评估血管构筑,超选造影确认微导管位置
3. 关键操作步骤
(1)微导管穿过瘘口,置于近端静脉引流段(瘘口下游2-3cm)
(2)高流量瘘口需用超大号HydroCoil搭建稳定篮,再填塞小规格弹簧圈
(3)逆行致密填塞,见对比剂滞留/血栓形成立即停止
(4)双向静脉引流需双侧出口均封堵
(5)部分弹簧圈推送丝较短,需移除止血阀完成解脱
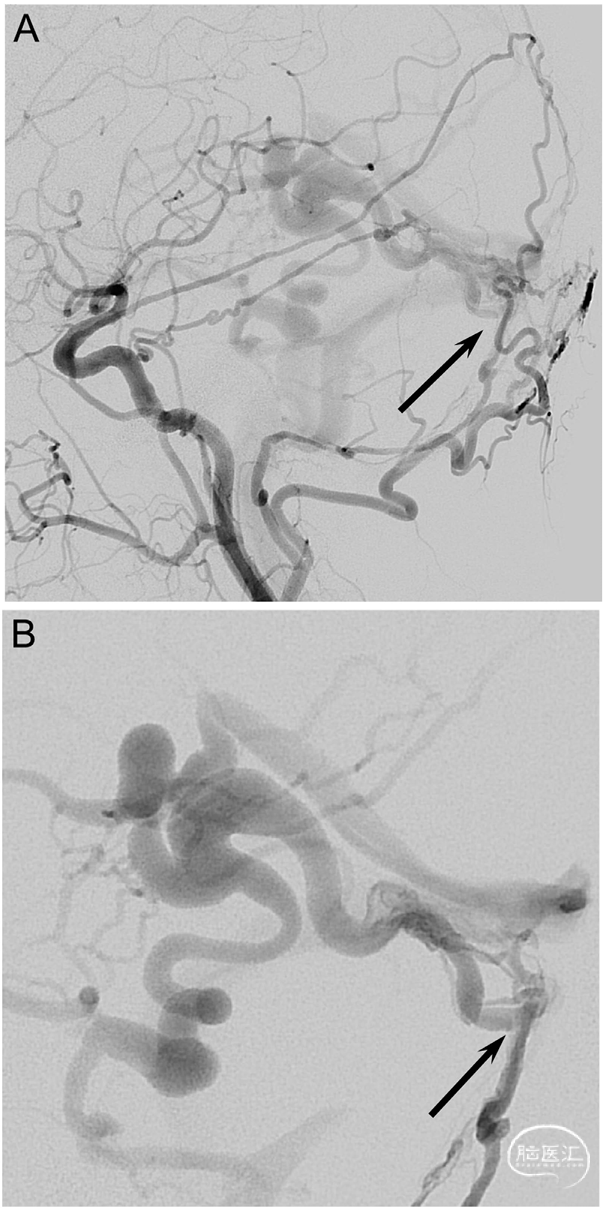
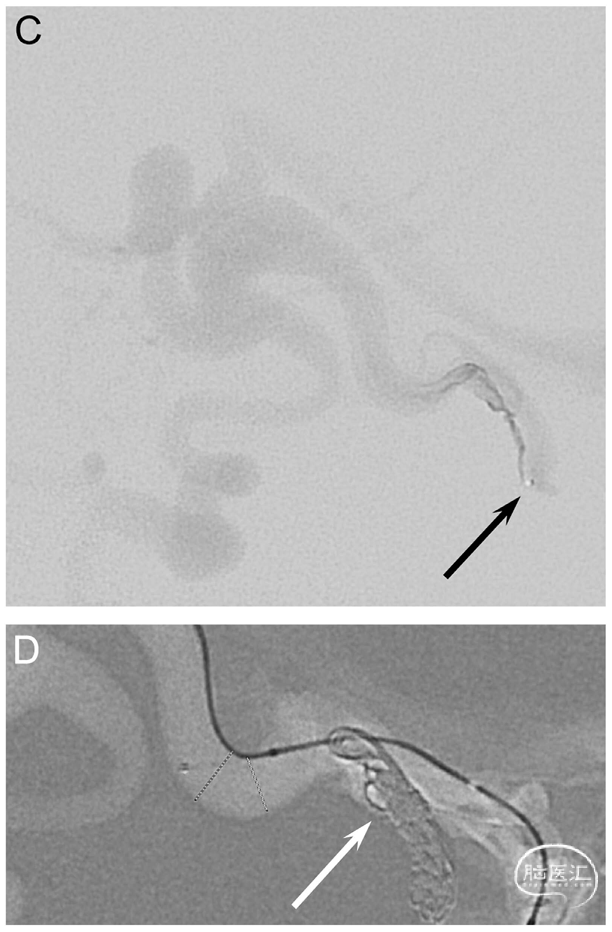
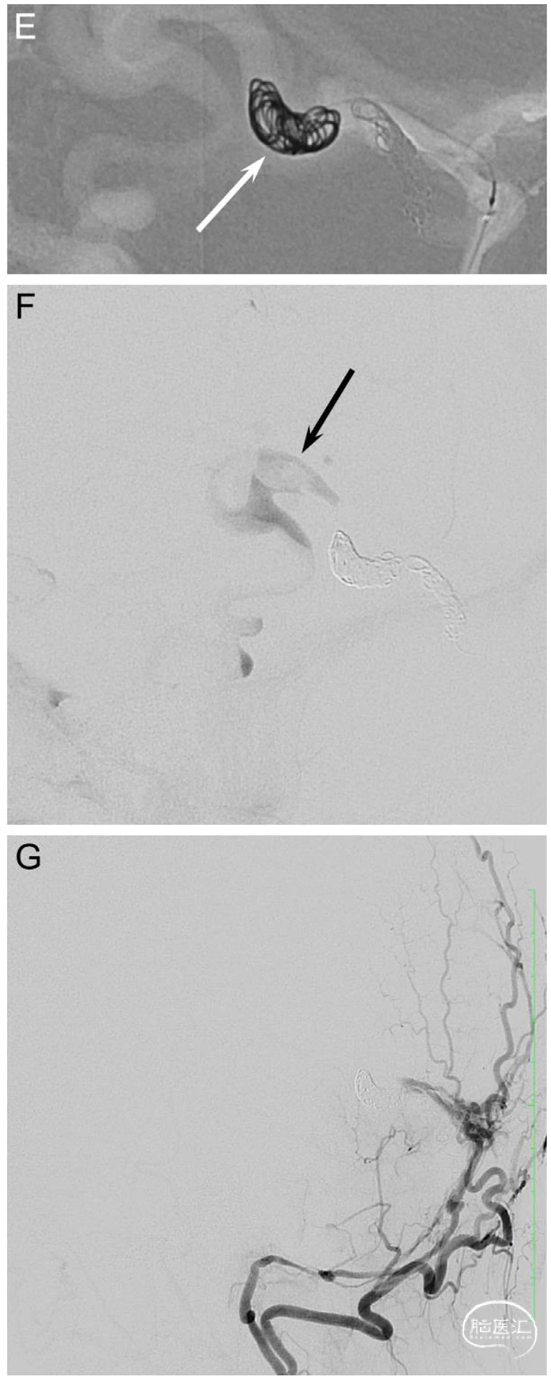
Fig. 1. A 52-year-old woman (patient no. 3) with headache and pulsatile tinnitus underwent an MRI showing dilated veins in the posterior fossa. A diagnostic DSA confirmed a high-grade tentorial DAVF near the confluence (Borden type III, Cognard type IV). A.-B. Left CCA and left selective posterior meningeal artery (PMA) injections in lateral views show a DAVF (arrow) with deep venous drainage and several venous ectasias. C. Lateral view showing the transfistulous approach performed via the left PMA using a triaxial system with a 5F Sofia and a 1.3F Headway™ Duo (Terumo Neuro) reaching the proximal venous outflow (arrow). D.-E. Roadmap in lateral views. The fistulous outflow consisted of two adjacent, first separately draining and then merging veins, both of which were tightly packed with coils (arrows). Due to the high flow, the 2nd and more enlarged distal portion (E) required an oversized HydroCoil18 (10 mm x 31 cm, Terumo Neuro) for a stable basket to be filled with smaller Target XL coils (Stryker). F. Late-phase left ICA control run in lateral view shows formation of thrombus in the dilated draining vein as a filling defect (arrow). G. Left occipital artery control run in lateral view shows complete occlusion of the arteriovenous shunting. Follow-up DSAs showed near-complete occlusion after 3 months and complete occlusion after 9 months (not shown).
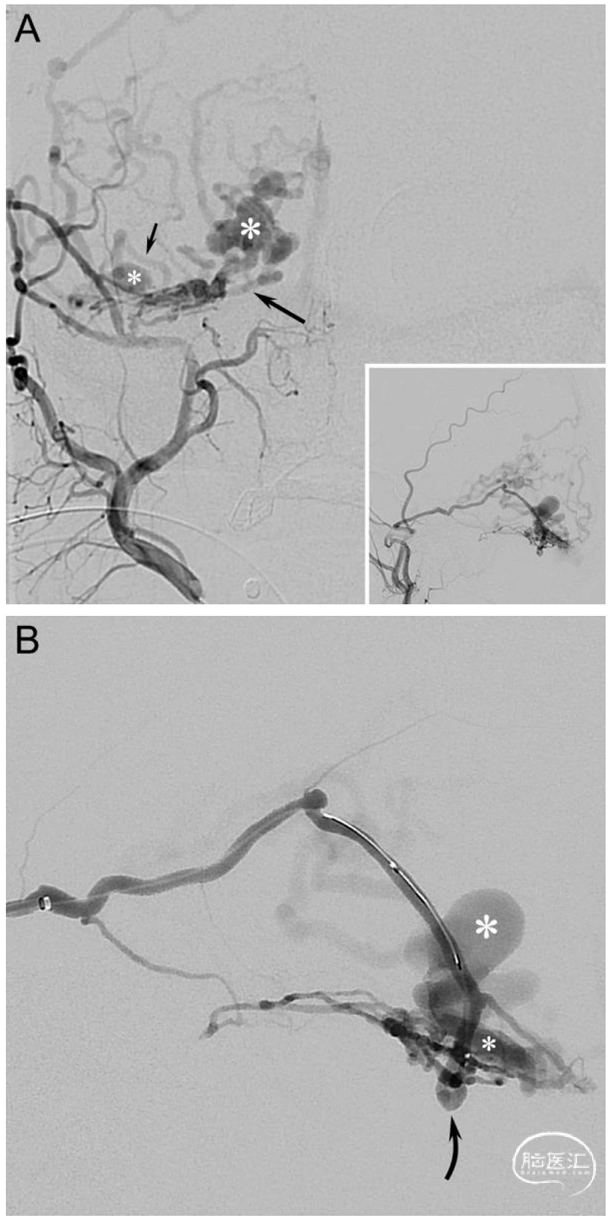
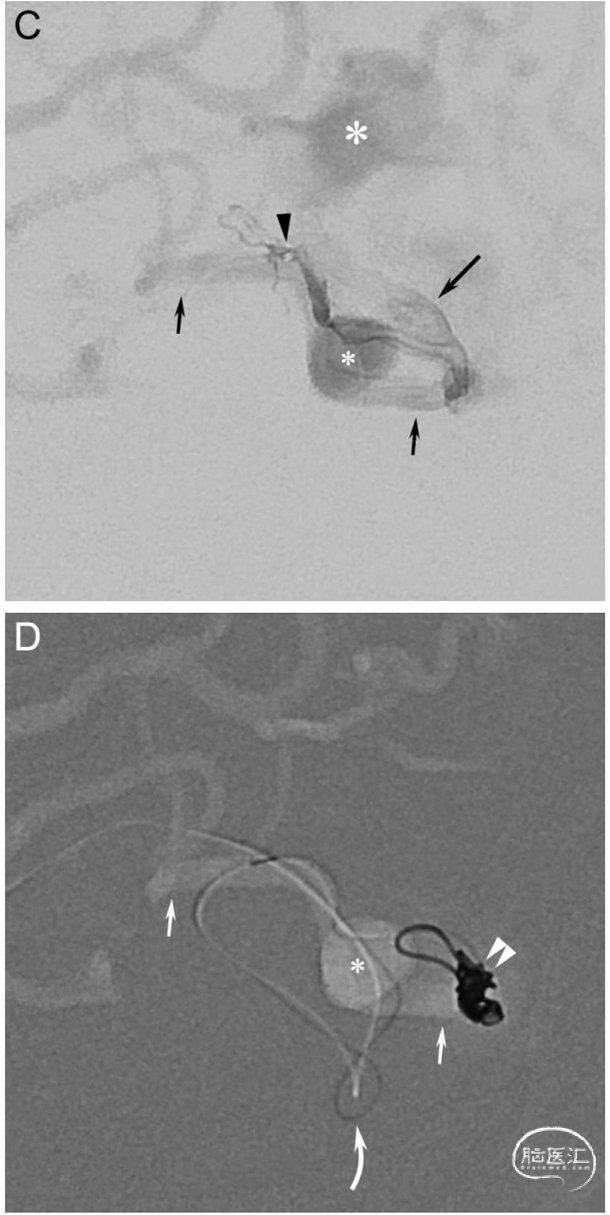
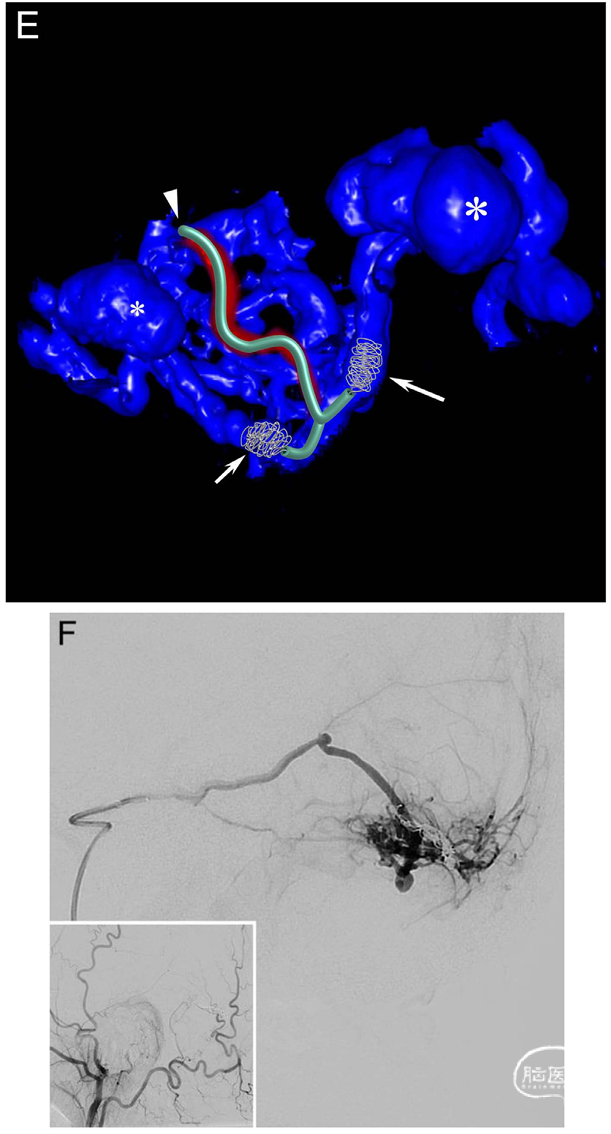
Fig. 2. A 60-year-old man (patient no. 2) presented with left-sided hemianopsia and headache due to an intracerebral hemorrhage in the right occipital lobe. A diagnostic DSA showed a high-grade tentorial DAVF (Borden type III, Cognard type IV). A. Right ECA injection in AP view shows the DAVF supplied mainly by an enlarged middle meningeal artery with arteriovenous shunting to medial (long arrow) and lateral (short arrow) venous drainage routes carrying several ectasias (medial: large asterisk, lateral: small asterisk). Insert: Right ECA injection in lateral view. B. Middle meningeal artery injection in lateral view shows that the main feeder (curved arrow) splits up into smaller pedicles before reaching the venous compartments. The medial venous ectasia (large asterisk) is located above the tentorium, while the lateral venous ectasia (small asterisk) is superimposed by the AV shunt. C. Lateral view of a superselective injection with the microcatheter tip (arrowhead) located distally in the main middle meningeal artery pedicle before entering the venous side. Both the medial (long arrow) and lateral (short arrows) venous drainage routes are visible with their medially (large asterisk) and laterally (small asterisk) located venous ectasias. D. Roadmap in lateral view shows that the 1.3F Headway™ Duo microcatheter (curved arrow) was navigated through the distal pedicle into the lateral draining vein (small arrows) first, where coils (double arrowhead) were deployed. After a minimal pullback and navigation into the opposite direction, coils were also deployed in the medial draining vein. Small asterisk: Venous ectasia on the lateral venous drainage route. E. Volume rendering technique (VRT) reconstruction based on a distal middle meningeal artery injection before coil deployment shows the pedicle (arrowhead) entering the initial venous segment, which divides into medial (long arrow) and lateral (short arrow) draining veins. The course of the microcatheter and the location of the coils are shown. Both the medial (large asterisk) and lateral (small asterisk) venous ectasias are visible. F. Control run in lateral view shows complete blockage of the arteriovenous shunting at the end of the procedure. Insert: Right ECA injection in lateral view shows stable occlusion of the DAVF after 3 months.
1. 影像学结果
✔ 完全解剖闭塞:4/5例
✔ 近全闭塞:1/5例(复杂镰幕型,分期治疗残余瘘为Borden/Cognard Ⅰ型低级别良性瘘)
✔ 自发闭塞:病例3术后3月近全闭塞,9月随访完全闭塞
2. 临床结果
✔ 临床治愈:4/5例
✔ 1例术前伴晚期痴呆、癫痫、静脉梗死后遗症,术后症状无改善(与基础病相关)
3. 治疗模式
✔ 3例:单术程TFA根治
✔ 1例:TFA联合PHIL液体栓塞
✔ 1例:分期TAE后行最终TFA
4. 随访方案
4例完成术后3个月DSA常规随访
● 无任何手术相关并发症(无卒中、出血、夹层、颅神经损伤、导管嵌顿)
● 无术后新发神经功能缺损
● 静脉端操作路径短,穿孔/出血风险更低;动脉入路更利于出血控制
● 无靶外栓塞、无导管嵌顿风险
● 精准封堵静脉瘘脚(foot of the vein,DAVF根治核心靶点)
● 可控性更强,单术程根治率高
● 避免LEA反流、充盈不全的缺陷
● 可联合LEA使用,适配复杂病例
● 不适用于多发分散瘘口的DAVF
● 不适用于供血动脉纤细、弥漫网状供血的DAVF(如Ⅰ型DAVF)
● 微导管无法穿过瘘口进入静脉腔时禁用
TFA重回临床视野,得益于:
✔ 新一代低剖面微导管(1.3F Headway Duo,工作长度167cm)
✔ 三轴系统支持
✔ 可完成既往难以实现的迂曲路径超选
![]()
声明:脑医汇旗下神外资讯、神介资讯、脑医咨询、Ai Brain 所发表内容之知识产权为脑医汇及主办方、原作者等相关权利人所有。
投稿邮箱:NAOYIHUI@163.com
未经许可,禁止进行转载、摘编、复制、裁切、录制等。经许可授权使用,亦须注明来源。欢迎转发、分享。
投稿/会议发布,请联系400-888-2526转3。
