


Review
History
•44 y/o female.
•Suffered from left upper limb numbness for 2 months. A right cavernous segment aneurysm was detected incidentally (w/o).
•Past medical history: HTN and DM for about 2 years, both controlled unsatisfactorily. Smoking for 20 years, not quitted.
•Medication: Aspirin; Valsartan; Metformin.
•NE: (-).
•44岁,女性。
•左上肢麻木2月。检查偶然发现右侧海绵窦段动脉瘤(没有图像)。
•既往史:高血压、糖尿病2年,均控制不佳;吸烟20余年,未戒烟。
•药物:阿司匹林;缬沙坦;二甲双胍。
•神经查体:-。
Figure 1 GIF. A right narrow-necked cavernous sinus segment aneurysm and a tiny wide-necked middle cerebral artery aneurysm incorporating the inferior trunk were observed.
图 1 GIF. 造影证实右侧颈内动脉海绵窦段窄颈动脉瘤,右侧大脑中动脉分叉部宽颈微小动脉瘤,动脉瘤累及大脑中动脉下干。
Figure 2 GIF. Two left middle cerebral artery aneurysms were visualized, with one incorporating the superior trunk and the other locating at the middle and inferior trunk bifurcation.
图 2 GIF. 造影证实左侧大脑中动脉2枚动脉瘤,一枚位于中动脉上干,另一枚位于中下干分叉部。
1
Strategy
Bilateral multiple middle cerebral artery aneurysms and a right cavernous segment aneurysm harboured rupture risks, which should be treated.
For the two left middle cerebral artery aneurysms: one incorporated the superior trunk and the other located on the middle and inferior trunk bifurcation. Stent assisted coiling technique will be adopted. A stent will be deployed in the middle trunk to cover the two aneurysms simultaneously (a stent could be deployed in the inferior trunk without the superior trunk aneurysm).
For the right tiny wide-necked regular middle cerebral artery aneurysm, simple Solitaire stenting technique was preferred.
Simple coiling will be adopted for the narrow-necked right cavernous segment aneurysm.
The left two middle cerebral artery aneurysms with a relative high treatment risk will be embolized first.
双侧大脑中动脉多发动脉瘤及右侧海绵窦段动脉瘤,有破裂风险,建议治疗。
左侧大脑中两枚动脉瘤:一枚仅累及上干起始部,另一枚位于中下干分叉部。采用支架辅助栓塞,计划将支架放置在中干,可同时覆盖两枚动脉瘤颈(若无上干起始部动脉瘤,可将支架在下干释放)。
右侧大脑中动脉宽颈微小动脉瘤,形态规则,可采用单Solitaire支架治疗。
右侧海绵窦段窄颈动脉瘤采用单纯弹簧圈栓塞技术。
左侧大脑中两枚动脉瘤,治疗风险相对较高,优先治疗。
2
Step 1. L-MCA ANs
Figure 3 GIF. Middle and inferior trunk bifurcation aneurysm measurements, size 1.92*1.09mm. General heparinization was performed. 6F Envoy DA guiding catheter was placed at the cavernous sinus segment. Echelon-10 45° microcatheter was navigated into the aneurysm sac. Insert a Target 360 2mm*3cm coil.
图 3 GIF. 右侧大脑中动脉中下干分叉部动脉瘤大小1.92*1.09mm。行全身肝素化。6F Envoy DA导引导管置于海绵窦段, Echelon-10 45° 微导管置于动脉瘤腔内,填入Target 360 2mm*3cm弹簧圈。
Figure 4 GIF. Angiogram did not demonstrate any bleeding or thrombosis.
图 4 GIF. 复查造影未见出血或栓塞。
Figure 5 GIF. A spiral curved Echelon 10 45° microcatheter was placed into the superior trunk aneurysm sac and a Prowler plus microcatheter into the middle trunk. Deployed a Solitaire 4mm*20mm stent via the Prowler plus and the Echelon 10 microcatheter was kicked out. Reshaped a Echelon 10 microcatheter into an “M”tip and navigated the microcatheter into the sac. Then inserted a Prime helical 1mm*3cm coil (aneurysm diameter 1.39mm).
图 5 GIF. Echelon 10 45°微导管头端塑螺旋弯后置于上干起始部动脉瘤腔内,Prowler plus微导管置于大脑中动脉中干远端。Solitaire 4mm*20mm支架于瘤颈部释放,栓塞微导管弹出动脉瘤腔。将Echelon 10微导管头端重新塑“M”型后置于动脉瘤腔内,填入一枚Prime helical 1mm*3cm弹簧圈(动脉瘤直径约1.39mm)。
Figure 6 GIF. The flow in the middle branch decreased due to thrombus, therefore Tirofiban 10ml was administered. Angiogram showed the aneurysms packed densely with parent artery patent. While vasospasm occurred in the proximal segment and Nimodipine 0.5ml was injected.
图 6 GIF. 复查造影中干分支血流减慢,考虑局部血栓形成。经导引导管给予替罗非班10ml。复查该侧颈内动脉造影证实动脉瘤不显影,载瘤动脉通畅。回撤导引导管至颈段,血管近端痉挛明显,经导引导管给予尼莫地平0.5ml。
Figure 7 GIF. The vasospasm improved and the aneurysms was densely packed.
图 7 GIF. 复查造影痉挛好转,动脉瘤致密栓塞。
3
Step 2. R-MCA ANs
Figure 8 GIF. The right middle cerebral artery aneurysm size 1*1mm. Prowler plus microcatheter was advanced into the inferior trunk via a Synchro-II microwire. Then deployed a Solitaire 4mm*20mm stent. Angiogram showed the parent artery straightened significantly and the tiny aneurysm was invisible.
图 8 GIF. 右侧大脑中动脉瘤大小约1*1mm。Prowler plus微导管在Synchro-II微导丝导引下置于大脑中动脉下干,瘤颈部释放Solitaire 4mm*20mm支架。复查造影载瘤动脉明显拉直,动脉瘤未见显影。
4
Step 3. R-ICA cavernous segment ANs

Figure 9 GIF. Right internal carotid artery cavernous segment aneurysm diameter 4.94mm. Echelon-10 45° microcatheter was navigated into the aneurysm sac. Insert 4 coils (TJWY-3D 5mm*20cm, TJWY-3D 2mm*4cm (x3)). Angiogram showed the dense packing of the aneurysm.
图 9 GIF. 右侧颈内动脉海绵窦段动脉瘤直径约4.94mm。Echelon-10 45° 微导管置于动脉瘤腔内,填入TJWY-3D 5mm*20cm, TJWY-3D 2mm*4cm (x3)共4枚弹簧圈,将动脉瘤致密栓塞。
Figure 10 GIF. The two aneurysms were both invisible and rotational DSA did not depicted any bleeding or thrombus.
图 10 GIF. 复查右侧颈内动脉造影右侧海绵窦段动脉瘤及大脑中动脉瘤不显影,旋转DSA未见出血或血栓形成。
Figure 11 GIF. No hemorrhage was observed from Dyna-CT.
图 11 GIF. Dyna-CT未见出血。
5
Post-operation
NE: GCS 15, eye movement normal, bilateral muscle strength normal, bilateral Babinski negative.
Medication: Tirofiban 6ml/h maintained for 48 hours. Dual antiplatelets and Atorvastatin were prescribed.
TEG: AA 100%, ADP 27.5%.
At discharge: Clopidogrel 75mg for 3 months and Aspirin 100mg for long term.
神经查体:GCS 15,眼球运动可,四肢肌力正常,双侧巴氏征阴性。
药物:替罗非班6ml/h维持48h;予口服双抗及阿托伐他汀。
血栓弹力图:阿司匹林抑制率100%,氯吡格雷抑制率27.5%。
出院:氯吡格雷75mg口服3月,阿司匹林100mg长期口服。
Figure 12 GIF. No recurrence pf the left middle and inferior trunk bifurcation aneurysm was observed while mild intra-stent stenosis was found by 12 month follow up angiogram.
图 12 GIF. 12月复查造影未见左侧大脑中动脉中下干分叉部动脉瘤复发,支架内可见轻度狭窄。
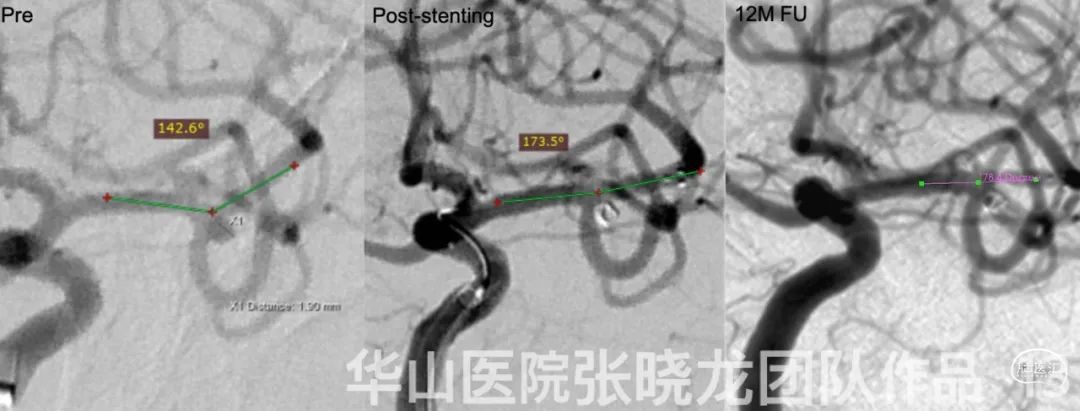
Figure 13. The left middle cerebral artery middle trunk straightened significantly by a Solitaire stent.
图 13. Solitaire支架将左侧大脑中动脉中干明显拉直。
Figure 14 GIF. Left superior trunk aneurysm was embolized densely by 12 month follow up.
图 14 GIF. 12个月随访左侧大脑中动脉上干动脉瘤致密栓塞。
Figure 15 GIF. Left internal carotid artery rotational DSA revealed mild intra-stent stenosis and did not demonstrate any relapsed aneurysm.
图 15 GIF. 左侧颈内动脉旋转造影提示支架内轻度狭窄,未见动脉瘤复发。
Video 1. No recurrence was found from the angiogram.
视频 1. 12月复查右侧两枚动脉瘤未见复发或残余。
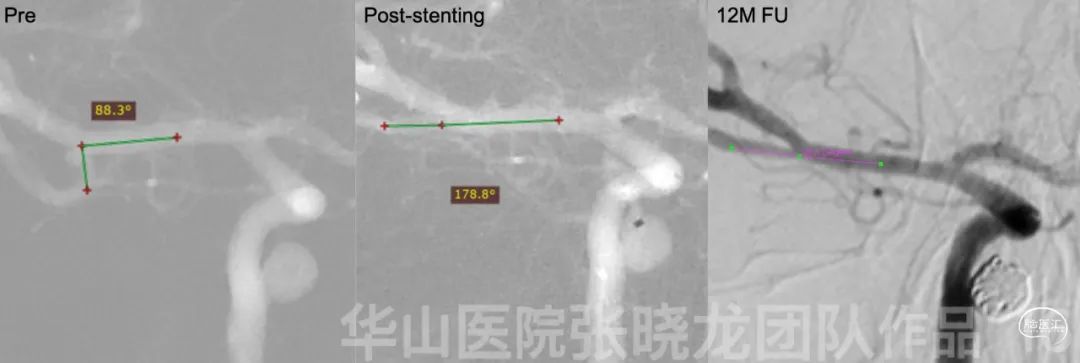
Figure 16. The right middle cerebral artery inferior trunk straightened obviously.
图 16. 右侧大脑中动脉下干明显拉直。
Video 2. Right internal carotid artery rotational DSA did not find any relapse of the aneurysms and the intracranial vessels remained intact by 12 month follow up.
视频 2. 12月复查右侧颈内动脉旋转造影未见动脉瘤残留,颅内血管完好。
6
Summary
Bilateral multiple middle cerebral artery aneurysms and a right cavernous segment aneurysm harboured rupture risks, which should be treated.
The left two middle cerebral artery aneurysms with a relative high treatment risk will be embolized first.
For the two left middle cerebral artery aneurysms: one incorporated the superior trunk and the other located on the middle and inferior trunk bifurcation. Stent assisted coiling technique was adopted. A stent was deployed in the middle trunk to cover the two aneurysms simultaneously (a stent could be deployed in the inferior trunk without the superior trunk aneurysm). Meanwhile the two aneurysms did not need dense packing because of a low recurrence risk.
A single large coil was selected for the left middle and inferior trunk bifurcation aneurysm because a large coil can form a stable basket and work as a stent.
For the right tiny wide-necked regular middle cerebral artery aneurysm (roughly 1mm), simple Solitaire stenting technique was preferred. By 12 month follow up, no recurrence was observed. A longer term follow up is still required.
Simple coiling was adopted for the narrow-necked right cavernous segment aneurysm.
Parent artery straightened by a Solitaire stent could lower the recurrence risk.
Unsatisfactory blood sugar control and smoking may be the hazardous factors of intra-stent stenosis. Continue statin and Aspirin.
Next follow up was scheduled in 2-3 years.
双侧大脑中动脉多发动脉瘤及右侧海绵窦段动脉瘤,有破裂风险,建议治疗。
左侧大脑中两枚动脉瘤,治疗风险相对较高,优先治疗。
左侧大脑中两枚动脉瘤:一枚仅累及上干起始部,另一枚位于中下干分叉部(主要累及下干) 。采用支架辅助栓塞,将支架放置在中干,可同时覆盖两枚动脉瘤颈(若无上干起始部动脉瘤,可将支架在下干释放)。这两枚小动脉瘤,复发风险低,无需致密栓塞。
左侧大脑中动脉中下干分叉部动脉瘤选用了一个大圈,考虑大圈成篮更稳定,同时有大圈代支架作用。
右侧大脑中动脉宽颈微小动脉瘤(大约1mm),形态规则,采用单Solitaire支架治疗。12个月随访该动脉瘤未见复发,但仍需更长期的随访结果。
右侧海绵窦段窄颈动脉瘤采用单纯弹簧圈栓塞技术。
Solitaire支架拉直载瘤动脉能降低动脉瘤复发风险。
血糖控制不佳和吸烟可能是支架内再狭窄的危险因素,建议继续他汀和阿司匹林治疗。
建议2-3年后随访。

点击或扫描上方二维码
查看更多“介入”内容
