


Our case
History
• Female, 71-year-old.
• 体格检查:(-)
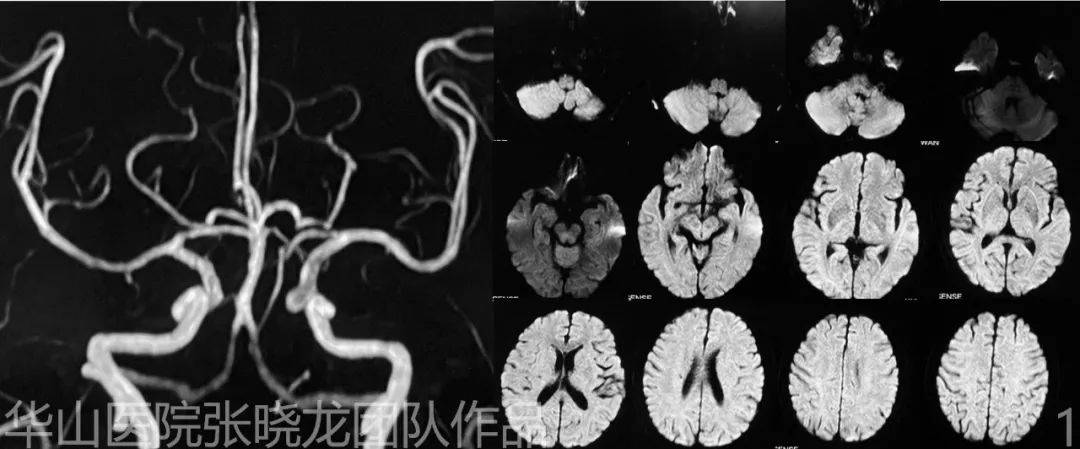
Figure 1. MRA shows a medial side of carotid-ophthalmic aneurysm. DWI shows no acute infarction. MRA可见一枚朝向内侧的颈眼动脉瘤。DWI未见急性梗死灶。

Figure 2. Two tiny aneurysms in ophthalmic segment of right ICA. 右侧颈内动脉眼段两枚小动脉瘤。
1
Strategy
• Two tandem ophthalmic aneurysms in the left ICA were revealed, one regular-shaped and wide-necked indicating a low rupture risk1, while the other is narrow-necked resulting in a high rupture risk1 which could be treated with simple coiling.
2
Operation
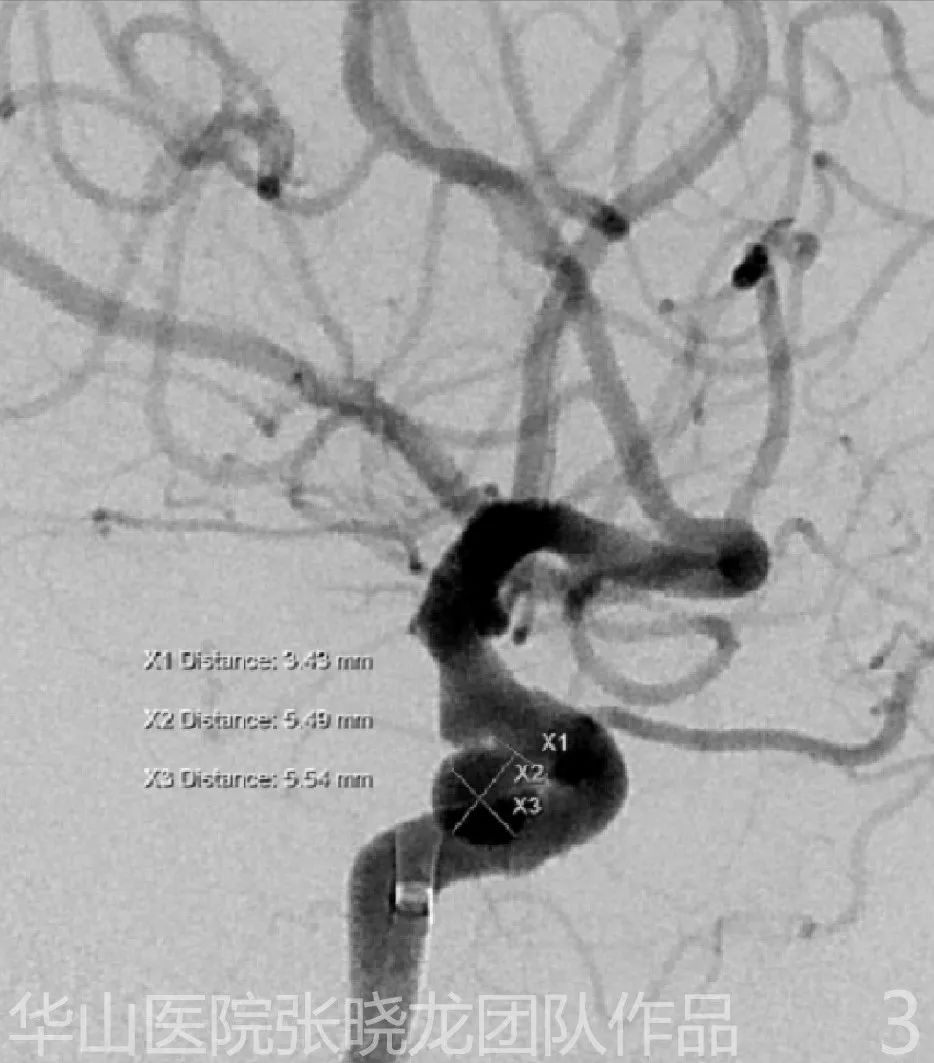
Figure 3. Maximal diameter: 5.5 mm. The working projection shows the necks of both aneurysms on a single image. 动脉瘤最大直径:5.5 mm。工作角度能在同一张图像上显示两枚动脉瘤的瘤颈。
Video 3. 6F Envoy DA was advanced as far as possible via microcatheter and microwire. General heparinization. Echelon-10 microcatheter tip was shaped into a medial spiral curve. 6F Envoy DA导引导管借助微导管和微导丝尽可能走远。全身肝素化。Echelon-10微导管头端塑形为向内侧的螺旋形。

Figure 4 GIF. MicroPlex 6mm*20cm for framing. MicroPlex 6mm*20cm成篮。
Figure 5 GIF. MicroPlex-10 5mm*15cm. MicroPlex-10 5mm*15cm。
Figure 6 GIF. HydroCoil 4mm*8cm. The first Hydrocoil was difficult to insert. We kept the tension of the microcatheter and waited several seconds before inserting. HydroCoil 4mm*8cm。第一枚Hydrocoil弹簧圈很难填入。我们保持微导管张力,等待几秒后再填入弹簧圈。

Figure 7 GIF. HydroCoil 3mm*8cm. HydroCoil 3mm*8cm。
Figure 8 GIF. HydroCoil 2mm*3cm. The microcatheter was kicked out. We retrieved the microcatheter and re-navigated it into the inflow tract. The last coil densely packed the aneurysm neck. HydroCoil 2mm*3cm。微导管脱出。我们取出微导管并将其重新送至流入道。最后一枚弹簧圈致密栓塞瘤颈。
Figure 9 GIF. Working projection angiography shows the densely packing of the aneurysm with parent artery patent. 工作角度血管造影可见动脉瘤致密栓塞,载瘤动脉通畅。
3
Post operation
Figure 10 GIF. Post-operative rotational angiography shows the intact of intracranial vessels. 术后旋转造影上颅内血管显示完整。
Figure 11 GIF. Post-operative Dyna CT shows no hemorrhage. 术后Dyna CT未见出血。
4
Summary
• Two tandem ophthalmic aneurysms in left ICA were revealed, one was regular-shaped and wide-necked indicating a low rupture risk, while the other is narrow-necked and therefore had a high rupture risk which could be treated with simple coiling.
• Large framing coil technique might decrease the recurrence rate while long term follow up DSA is necessary.
• Guiding catheter should be advanced across the petrosal curve as far as possible which can improve the maneuverability.
• The Hydrocoil is stiff and therefore difficult to insert. We kept the tension of the microcatheter and waited a few seconds to insert the third coil, a Hydrocoil 4*8.
• Two tiny carotid-ophthalmic aneurysms of the right ICA should be followed up.
• 左侧颈内动脉可见两枚串联的颈眼动脉瘤。其中一枚形状规则的宽颈动脉瘤破裂风险低;而另一枚窄颈动脉瘤破裂风险高,可行单纯栓塞治疗。
• 大圈成篮技术可能降低复发率,但需要长期的DSA随访。
• 导引导管应尽量通过岩骨段并走远,从而提高可操作性。
• Hydrocoil弹簧圈较硬,因此很难填入。我们保持微导管张力,等待几秒后填入第三枚弹簧圈(Hydrocoil 4mm*8cm)。
• 右侧颈内动脉眼段的两枚小动脉瘤应继续随访。
