



2020年5月14日,Balt宣布已获得美国FDA研究性器械豁免(IDE)的批准,启动运用Squid栓塞脑膜中动脉治疗慢性硬脑膜下血肿(STEM)临床研究。
慢性硬脑膜下血肿(cSDH)是一种主要影响老年人的常见疾病。近期的一项由退伍军人事务部发起的cSDH研究发现患病率在每十万人79.4例。作者预测cSDH在美国老兵和平民人群的发病率将分别达到每十万人121.4例和17.4例。到2030年,美国每年大约新发60,000例慢性硬脑膜下血肿。“我们对于有机会参加研究Squid液体栓塞剂作为该普遍而致残性神经疾病的一种微创治疗方案而感到兴奋。”Dr. David Fiorella如是说。
该临床试验是一项全球多中心前瞻性随机对照研究。共同主要研究者Dr. Adam Arthur (Semmes-Murphey Neurologic and Spine Institute and University of Tennessee Health Sciences Center) 和 Dr. David Fiorella (Stony Brook University Medical Center) 做了大量的工作来设计这一有意义的研究。
研究目的是为了展现运用Squid液体栓塞剂栓塞脑膜中动脉(MMA)干预外科治疗和非外科治疗患者的cSDH的安全性和有效性。Dr. Arthur说道:“这是一种影响了许多人尤其是老年人的疾病。现有治疗方法普遍未经过严谨的临床研究,且经常需要病人接受创伤性手术并长期滞留在ICU内。”
患者经常表现出局灶性神经症状,非局灶性认知症状和整体功能障碍。“STEM研究将使我们在如何帮助这些患者,如何最好地治疗老年人痴呆和残疾以及寻找逆转原因方面掌握大量知识” ,Dr. Arthur补充道。
Dr. Fiorella 继续说:“我们在使用液体栓塞剂联合外科手术治疗和单独治疗患有cSDH的病人时均观察到许多出乎意料的影像学和临床改善。我们希望本随机对照研究将提供确实证据证明使用Squid栓塞脑膜中动脉不仅能够改善外科手术预后,还能为患者提供一种微创血管内治疗手段,不再需要急诊开颅手术。一大组病人的预后改善将代表一次巨大的进步。”
Balt CEO Pascal Girin 评论道:“此次IDE批准STEM研究是Balt的重要里程碑,这将是Balt在美国的第一个前瞻性研究,也代表着我们不断投入临床研究来解答目前临床上未解难题的承诺。”

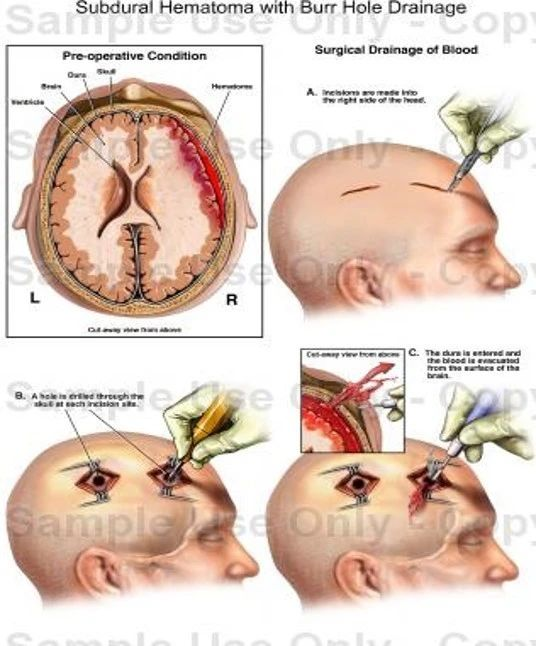
慢性硬膜下血肿 (cSDH):
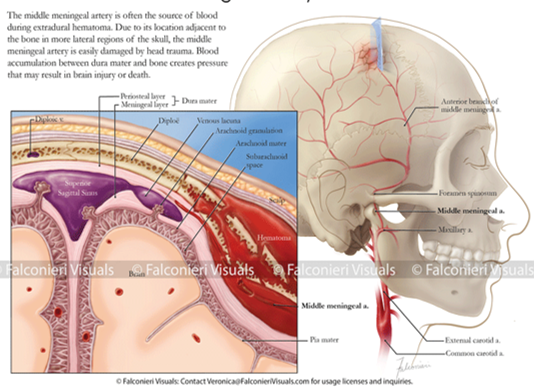
• 在成人中是一种缓慢积累的大脑表面出血,导致大脑受压迫,患者表现为局灶性神经症状,认知障碍或广泛性神经功能障碍。
• 病因:创伤性,自发性(尤其是在抗凝/抗血小板治疗的病人身上)。

cSDH当前治疗存在诸多问题:
• 保守治疗:病人症状持续存在,神经功能缺失,不能独立生活/较低的生活质量;
• 手术治疗: 高死亡率(30%)和高复发率(15%) 。11%-19%的患者癫痫发作,围手术期死亡率:1.2%至11%,术后1年死亡率:高达32%;
• 治疗决策主要依赖专家经验,尚无严格指南/标准。诸多问题导致只有15 - 20%的病人得到手术治疗。
老龄化带来cSDH增加:
•专家预测:一旦有20%到25%的人口年龄超过65岁,CSDH将超过原发性和转移性脑肿瘤,成为2030年最常见的神经外科疾病。
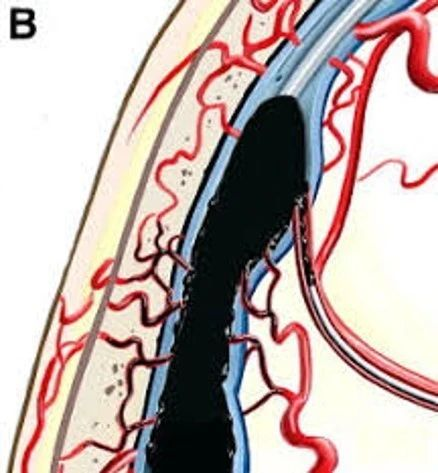
介入治疗的优势:
•亚洲的一些研究中心率先使用PVA颗粒介入栓塞脑膜中动脉(MMA)--在2018年发表的一篇文章中,对72名患者进行介入治疗的前瞻性研究显示,经PVA栓塞MMA治疗患者的获益,经治疗组再手术率较低,而保守治疗组再手术率较高。
•血肿再增加对比:栓塞组2.2% VS 标准治疗组27.5%。使用Squid(Balt)替代PVA颗粒,极有可能达到同等或(更有可能)更好的治疗效果。
参考文献
1.Balser D, Farooq S, Mehmood T, Reyes M, Samadani U. Actual and projected incidence rates for chronic subdural hematomas in united states veterans administration and civilian populations. Journal of neurosurgery. 2015;123:1209-1215
2.Kalamatianos T, Stavrinou LC, Koutsarnakis C, Psachoulia C, Sakas DE, Stranjalis G. Plgf and svegfr-1 in chronic subdural hematoma: Implications for hematoma development. Journal of neurosurgery. 2013;118:353-357
3.Stanisic M, Aasen AO, Pripp AH, Lindegaard KF, Ramm-Pettersen J, Lyngstadaas SP, et al. Local and systemic pro-inflammatory and anti-inflammatory cytokine patterns in patients with chronic subdural hematoma: A prospective study. Inflamm Res. 2012;61:845-852
4.Santarius T, Kirkpatrick PJ, Kolias AG, Hutchinson PJ. Working toward rational and evidence-based treatment of chronic subdural hematoma. Clin Neurosurg. 2010;57:112-122
5.Baechli H, Nordmann A, Bucher HC, Gratzl O. Demographics and prevalent risk factors of chronic subdural haematoma: Results of a large single-center cohort study. Neurosurg Rev. 2004;27:263-266
6.Kang J, Whang K, Hong SK, Pyen JS, Cho SM, Kim JY, et al. Middle meningeal artery embolization in recurrent chronic subdural hematoma combined with arachnoid cyst. Korean J Neurotrauma. 2015;11:187-190
7.Hirai S, Ono J, Odaki M, Serizawa T, Nagano O. Embolization of the middle meningeal artery for refractory chronic subdural haematoma. Usefulness for patients under anticoagulant therapy. Interv Neuroradiol. 2004;10 Suppl 2:101-104
8.Hashimoto T, Ohashi T, Watanabe D, Koyama S, Namatame H, Izawa H, et al. Usefulness of embolization of the middle meningeal artery for refractory chronic subdural hematomas. Surg Neurol Int. 2013;4:104
9.Ishihara H, Ishihara S, Kohyama S, Yamane F, Ogawa M, Sato A, et al. Experience in endovascular treatment of recurrent chronic subdural hematoma. Interv Neuroradiol. 2007;13 Suppl 1:141-144
10.Ban SP, Hwang G, Byoun HS, Kim T, Lee SU, Bang JS, et al. Middle meningeal artery embolization for chronic subdural hematoma. Radiology. 2018;286:992-999
11. Huang KT, Bi WL, Abd-El-Barr M, et al The neurocritical and neurosurgical care of subdural hematomas. Neurocrit Care. 2016;24(2):294-307.
12. Kolias AG, Chari A, Santarius T, Hutchinson PJ. Chronic subdural haematoma: modern management and emerging therapies. Nat Rev Neurol. 2014;10(10):570-578.
13. Schmidt L, Gortz S, Wohlfahrt J, Melbye M, Munch TN. Recurrence of subdural haematoma in a population-based cohort-risks and predictive factors. PLoS One. 2015;10(10):e0140450.
14. Morris NA, Merkler AE, Parker WE, et al Adverse outcomes after initial non-surgical management of subdural hematoma: a population-based study. Neurocrit Care. 2016;24(2):226-232.
15. Meagher RJ. Subdural hematoma. Medscape. 2017.
16. Tabuchi S, Kadowaki M. Chronic subdural hematoma in patients over 90 years old in a super-aged society. J Clin Med Res. 2014;6(5):379-383.
17. Balser D, Rodgers SD, Johnson B, Shi C, Tabak E, Samadani U. Evolving management of symptomatic chronic subdural hematoma: experience of a single institution and review of the literature. Neurol Res. 2013;35(3):233-242.
18. Guha D, Coyne S, Macdonald RL. Timing of the resumption of antithrombotic agents following surgical evacuation of chronic subdural hematomas: a retrospective cohort study. J Neurosurg. 2016;124(3):750-759.

